Specialist assessment and treatment planning for kidney tumours including kidney preserving robotic surgery.
A kidney tumour can feel frightening, but not every kidney mass behaves the same way
Most kidney tumours are found unexpectedly during ultrasound, CT or MRI scans performed for another reason. Many are small and slow-growing, while others need active treatment.
The first step is to understand the size, position and complexity of the tumour, how well each kidney is working, and whether treatment should involve surveillance, kidney-preserving surgery or removal of the whole kidney.
Mr Mohammed Aldiwani offers specialist private assessment for kidney cancer and kidney tumours in Leeds, with expertise in robotic kidney surgery and nephron-sparing surgery where suitable.

How kidney tumours are assessed
A clear plan starts with understanding the scans, the kidney function, and the safest treatment options for the individual patient.

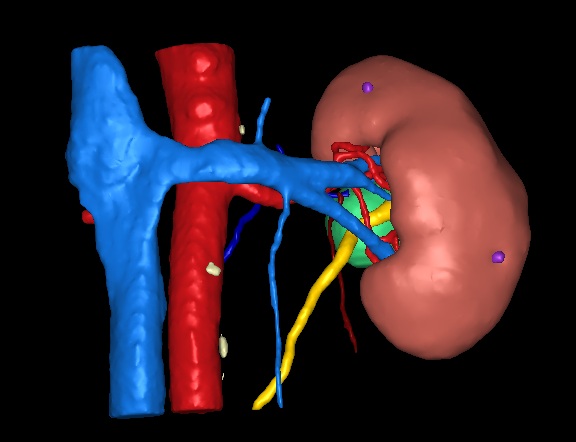
Review of imaging
Blood tests
Blood tests help assess how well the kidneys are working and whether preserving kidney tissue is especially important.
Biopsy
An ultrasound guided needle biopsy sample may be organised if the exact nature of the tumour is likely to influence treatment planning
Treatment Plan
Treatment may include surveillance, ablation, partial nephrectomy or radical nephrectomy.
Types of kidney tumour
A “kidney tumour” is a broad term. It does not always mean kidney cancer, and not all kidney cancers behave in the same way.
Some masses arise from the kidney tissue itself, such as renal cell carcinoma (RCC). Others may be benign, such as oncocytoma or angiomyolipoma. Some are complex cysts that need risk assessment rather than immediate surgery. A separate group arises from the lining of the kidney drainage system and ureter; this is called transitional cell carcinoma or upper tract urothelial carcinoma.
Renal Cell Carcinoma
Renal cell carcinoma, often shortened to RCC, is the most common type of kidney cancer. It usually starts in the kidney tissue itself and may be found incidentally on an ultrasound, CT or MRI scan.
Most small incidental RCC tumours are slow growing and non aggressive in the early stages.
Treatment depends on the size and position of the tumour and may include active surveillance, partial nephrectomy, radical nephrectomy, ablation or systemic treatment in more advanced cases.
When suitable, kidney-preserving treatment is considered
Benign kidney tumours
Around 10-20% of kidney tumours are benign, meaning they are not cancer. Examples include oncocytoma and angiomyolipoma.
A benign tumour may still need careful assessment because scans cannot always confirm the diagnosis with certainty. In selected cases, biopsy, surveillance or treatment may be recommended.
Complex kidney cysts
Kidney cysts are common and are usually harmless. However, some cysts have complex features such as thick walls, internal divisions or solid-looking areas.
Evaluation is primarily with CT imaging. Rarely biopsies are utilised.
Complex cysts are often classified using the Bosniak system (graded 1-4), which helps estimate the risk of cancer and guide whether surveillance or treatment is needed.
TCC / Upper Tract Urothelial Carcinoma
Some cancers found near the kidney do not start in the kidney tissue itself. Transitional cell carcinoma, also called upper tract urothelial carcinoma, can arise from the lining of the renal pelvis or ureter and is part of the same family as most bladder tumours.
This behaves differently from RCC and requires a thorough evaluation including cystoscopy and CT Urography. A urine cytology, ureteroscopy and biopsy may be required if there is doubt in the diagnosis.
Treatment often involves robotic nephroureterectomy or kidney-sparing approaches in selective cases.
For patients who are suitable for surgery, robotic kidney surgery may be used for selected kidney cancers and complex kidney conditions.
Treatment options for RCC
The right option depends on tumour stage, size, tumour position, kidney function, general health and patient preference.
Active surveillance
For many small tumours, careful monitoring with repeat imaging may be appropriate with a view to active treatment if they demonstrate change.
Many smaller tumours never require treatment, especially in older patients.
Kidney biopsy
A small sample may be taken when the diagnosis is uncertain or the result would change management.
Robotic partial nephrectomy
The tumour is removed while aiming to preserve healthy kidney tissue.
Traditionally a riskier operation, robotic techniques have made this the gold standard where it is feasible.
Radical nephrectomy
The whole kidney is removed when this is safer or more appropriate.
Some kidney function loss is sacrificed although the operation is typically straight forward.
Ablation
Selected small tumours may be treated using heat or cold through image-guided techniques.
It is performed under a full anaesthetic by a radiologist and is quite effective with shorter recovery time than surgery.
Partial vs Radical Nephrectomy
One of the key decisions in kidney cancer surgery is whether the tumour can be removed while preserving the rest of the kidney.
A partial nephrectomy removes the tumour with a thin margin of surrounding tissue, aiming to save as much healthy kidney as possible. A radical nephrectomy removes the whole kidney and may be the simpler option, particularly when the tumour is large, central, close to major blood vessels, or too complex to remove separately.
Many patients live well with one healthy kidney. However, kidney function may reduce with age, and conditions such as diabetes, high blood pressure or chronic kidney disease can place extra strain on the remaining kidney. Therefore, where it is safe and appropriate, kidney-preserving surgery is preferred to maintain long-term kidney reserve.
Partial Nephrectomy
A partial nephrectomy removes the kidney tumour while preserving the remaining healthy kidney. It is preferred wherever it is feasible depending on size, position and complexity.
Benefits
- ✓
Usually preferred for small or localised kidney tumours
- ✓
Helps preserve long-term kidney function
- ✓
Performed robotically
- ✓
Especially relevant if kidney reserve is already reduced
Key risks and trade-offs
Partial nephrectomy is more kidney-preserving, but it can be technically more complex than removing the whole kidney.
Important risks include bleeding or urine leakage from the cut surface of the kidney, the need for further treatment, or conversion to radical nephrectomy if preserving the kidney is not safe.
Robotic partial nephrectomy is very safe in expert hands.
Our complications rates for bleeding and urine leak are less than 1 in 100 cases.
Radical Nephrectomy
A radical nephrectomy removes the entire kidney, usually with surrounding fatty tissue. It may be safest when kidney preservation would carry excessive risk.
Benefits
- ✓Technically more straightforward than partial nephrectomy
- ✓May be safer for central or very complex tumours
- ✓Can often be performed using a robotic or keyhole approach
- ✓Less concern or risk of incomplete removal
Key risks and trade-offs
Radical nephrectomy can be the safer cancer operation when the tumour is large or complex, but it means losing the whole kidney.
Important risks include bleeding, infection, injury to nearby organs, blood clots, hernia, anaesthetic risks and reduced overall kidney reserve.
Long-term kidney function depends on how well the remaining kidney works.
Why choose Mr Aldiwani for partial nephrectomy?
Mr Mohammed Aldiwani is a high-volume surgeon with fellowship training in complex robotic kidney cancer surgery. He is one of the few surgeons nationally who routinely performs both retroperitoneal robotic surgery and the standard transperitoneal approach, allowing the surgical route to be tailored to the position of the tumour, the patient’s anatomy and any previous abdominal surgery.
The retroperitoneal approach offers direct access to the kidney without entering the abdominal cavity. This has been associated with reduced blood loss, shorter operating time and faster recovery compared with traditional approaches.
Mr Aldiwani’s outcomes are prospectively audited, with a greater than 90% trifecta rate for robotic partial nephrectomy. This means that surgery achieved clear surgical margins, no significant complications and low ischaemia time.
If you have been advised to have a radical nephrectomy, or you are wondering whether your tumour may be suitable for kidney-preserving surgery, you can arrange a specialist second opinion to review your scans and discuss whether partial nephrectomy may be appropriate.
Fellowship trained
Advanced Robotic fellowship training at Frimley Renal Cancer Centre and Royal Marsden Hospital, London. Royal College of Surgeons Accredited.
Retroperitoneal expertise
Direct-access robotic surgery for faster recovery. Mr Aldiwani is one of a few surgeons nationally routinely performing this approach for >90% of cases. See more.
High-volume robotic surgeon
High volume surgical practice with focus on partial nephrectomy, nephrectomy, nephro-ureterectomy, pyeloplasty and ureteric reconstruction.
>90% trifecta rate
Prospectively audited outcomes: clear margins, no significant complications and low ischaemia time.
Frequently asked questions
Common questions about kidney tumours, kidney-preserving surgery, robotic surgery and arranging a private consultation.
What happens after a kidney tumour is found?
You will usually have a detailed review of your scan, kidney function and general health. The aim is to understand the nature of the mass and the options available based on your individual circumstances. A treatment plan is proposed and discussed in a multi-disciplinary team meeting.
What symptoms can be caused by renal tumours?
Usually none. Especially smaller tumours which are nearly always chance findings.
Very large and more advanced tumours may cause pain, blood in the urine, fatigue or symptoms from sites it has spread to.
Is a tumour biopsy always needed?
Not always. Many kidney cancers are treated based on imaging appearances. For smaller tumours (<4cm), there is 1 in 5 chance the tumour is benign (not cancer). A biopsy may be helpful when the result would change the treatment plan. It is often considered in cases of bilateral tumours or higher risk patients where surgrey is preferably avoided.
Do all tumours need treatment?
No. Some small kidney tumours can be monitored carefully, particularly if they are slow-growing or if surgery carries higher risk. Other tumours are better treated actively.
Do benign tumours need treatment?
Often they do not, however in the case of diagnostic uncertainty, growing tumours and young patients sometimes partial nephrectomy is performed.
Is partial nephrectomy a risky operation?
Not as before. Historically, partial nephrectomy has been associated with complication rates of 10-20%. In expert hands, with robotic precision, the risk of bleeding and urine leak is considerably less. In Mr Aldiwani’s series, major complications are very rare (<2%).
How much kidney remains after partial nephrectomy?
Nearly all of it. A partial nephrectomy only involves removing the tumour with a very thin margin of normal kidney. This means minimal disruption to the normal kidney and its blood flow.
Is there a role for surgery if my tumour has already spread?
This is a complex area and requires a multi-disciplinary approach with oncologist and radiologist. Historically, surgical removal of the kidney was performed even if the cancer has spread. Modern cancer drugs have meant this only occurs in specific settings such as if there are symptoms from the kidney cancer or very little disease that has escaped.
How long does one stay in hospital after robotic kidney cancer surgery?
Most patients remain in hospital for only 1-2 nights.
What is the recovery time after surgery?
Patient experience of recovery can vary. As a guide, typical recovery is made with normal activities resumed around 4-6 weeks.
Does Mr Aldiwani treat upper tract urothelial cancer/TCC?
Yes. In addition to expertise in partial nephrectomy, Mr Aldiwani performs fully robotic nephro-ureterectomy for relevant patients.
Mr Aldiwani also treats eligible patients with lower risk tumours using endoscopic laser ablation.
Can I have robotic surgery privately in Leeds?
Yes. Since mid-2026, private robotic surgery has been available in Leeds, with the arrival of the first private surgical robot in Yorkshire.
Suitability depends on your scans, diagnosis, tumour position and overall health.
What should I bring to my consultation
Please bring or send CT, MRI or ultrasound reports, clinic letters, blood test results and details of previous abdominal surgery. Access to the actual scan images is very helpful..
Can I get a second opinion about kidney cancer surgery?
Yes. A second opinion can be helpful if you have been offered kidney removal and want to know whether kidney-preserving surgery or robotic surgery may be suitable.
Do you see patients from other regions?
Yes. A remote consultation can be organised initially to review imaging and provide an opinion. Surgery takes place in Leeds Spire Hospitals using the state of the art Da Vinci Xi Surgical robot.
Arrange a specialist consultation
For an individualised assessment about kidney cancer including second opinions; robotic surgery opinions, retroperitoneal access suitability or complex upper tract conditions, then please contact us to arrange an appointment.
© Yorkshire Urology Clinic. All Rights Reserved